
Overview
A heel spur is a hook that can form on the calcaneus (heel bone) and can also be related to plantar fasciitis (inflammation of the tissue in the foot?s arch). People who have plantar fasciitis often develop heel spurs. Middle-aged men and women are more prone to heels spurs, but all age groups can be afflicted. Heel spurs can be found through an x-ray, revealing a protruding hook where the plantar fascia is located.
Causes
A major cause of heel spur pain comes from the development of new fibrous tissue around the bony spur, which acts as a cushion over the area of stress. As this tissue grows, a callus forms and takes up even more space than the heel spur, leading to less space for the thick surrounding network of tendons, nerves, ligaments and supporting tissue. These important structures in the foot have limited space because of calcium or tissue buildup, which leads to swelling and redness of the foot, and a deep throbbing pain worsened with exercise.

Symptoms
Symptoms of heel spur syndrome often include pain early in the morning or after rest, as you take the first few steps. It may also include severe pain after standing or walking long hours, especially on hard cement floors. Usually more pain exist while wearing a very flat soled shoe. A higher heel may actually relieve the pain as an arch is created. The pain is usually sharp, but can also be a dull ache. The pain may only be at the bottom of the heel, or may also travel along the arch of the foot.
Diagnosis
A thorough medical history and physical exam by a physician is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
In case of heel spurs rest is most important. Active sports, running, long walks etc should be avoided to start with. If you?re in a job that requires a lot of standing, take a few days off work. Rest (or reduced activity) is essential to allow the inflammation from becoming aggrevated. Furthermore, you can use ice packs (placed on the heel for 5-10 minutes) to ?cool down? the inflamed area. You may take anti-inflammatory medication or apply a topical inflammatory (i.e. a cream) to help reduce inflammation. In addition, there are some simple exercises that should be done daily to help relieve heel spur pain.
Surgical Treatment
Usually, heel spurs are curable with conservative treatment. If not, heel spurs are curable with surgery, although there is the possibility of them growing back. About 10% of those who continue to see a physician for plantar fascitis have it for more than a year. If there is limited success after approximately one year of conservative treatment, patients are often advised to have surgery.
 Overview
Overview Symptoms
Symptoms Overview
Overview Symptoms
Symptoms The term "hallux valgus" or "hallux abducto-valgus" are the most commonly used medical terms associated with a bunion anomaly, where "hallux" refers to the great toe, "valgus" refers to the abnormal angulation of the great toe commonly associated with bunion anomalies, and "abductus/-o" refers to the abnormal drifting or inward leaning of the great toe towards the second toe, which is also commonly associated with bunions. It is important to state that "hallux abducto" refers to the motion the great toe moves away from the body's midline. Deformities of the lower extremity are usually named in accordance to the body's midline, or the line bisecting the body longitudinally into two halves. In more severe cases, the hallux continuing in the abductus fashion eventually either overlaps or underlaps subsequent lesser (small) toes especially the second (adjacent toe).
The term "hallux valgus" or "hallux abducto-valgus" are the most commonly used medical terms associated with a bunion anomaly, where "hallux" refers to the great toe, "valgus" refers to the abnormal angulation of the great toe commonly associated with bunion anomalies, and "abductus/-o" refers to the abnormal drifting or inward leaning of the great toe towards the second toe, which is also commonly associated with bunions. It is important to state that "hallux abducto" refers to the motion the great toe moves away from the body's midline. Deformities of the lower extremity are usually named in accordance to the body's midline, or the line bisecting the body longitudinally into two halves. In more severe cases, the hallux continuing in the abductus fashion eventually either overlaps or underlaps subsequent lesser (small) toes especially the second (adjacent toe).




 The Achilles tendon connects the muscles in the back of your lower leg to your heel bone. It allows you to move your foot down (?step on the gas? motion). This movement is essential for walking, running, and jumping. A sudden strong contraction of the lower leg (such as when playing sports) can partially tear or rupture the Achilles tendon. This injury is more likely if there is prior injury or inflammation of that tendon from prior stress. You may feel a pop or snap, or like you have been kicked. An Achilles tendon tear will cause local swelling and pain and difficulty in walking. A complete Achilles rupture is usually treated with surgery to attach the torn ends of the tendon. This is followed by 6-8 weeks in a walking cast, boot, or splint. Nonsurgical treatment is an option, but it will take longer to heal and the risk of repeat rupture is greater. With either type of treatment, you will need a physical therapy program to strengthen your Achilles tendon. It will take 4-6 months to return to your former level of activity. Causes The most common cause of a ruptured Achilles' tendon is when too much stress is placed through the tendon, particularly when pushing off with the foot. This may happen when playing sports such as football, basketball or tennis where the foot is dorsiflexed or pushed into an upward position during a fall. If the Achilles' tendon is weak, it is prone to rupture. Various factors can cause weakness, including corticosteroid medication and injections, certain diseases caused by hormone imbalance and tendonitis. Old age can also increase the risk of Achilles' tendon rupture. Symptoms Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel. An inability to bend your foot downward or "push off" the injured leg when you walk. An inability to stand up on your toes on the injured leg. A popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months.
The Achilles tendon connects the muscles in the back of your lower leg to your heel bone. It allows you to move your foot down (?step on the gas? motion). This movement is essential for walking, running, and jumping. A sudden strong contraction of the lower leg (such as when playing sports) can partially tear or rupture the Achilles tendon. This injury is more likely if there is prior injury or inflammation of that tendon from prior stress. You may feel a pop or snap, or like you have been kicked. An Achilles tendon tear will cause local swelling and pain and difficulty in walking. A complete Achilles rupture is usually treated with surgery to attach the torn ends of the tendon. This is followed by 6-8 weeks in a walking cast, boot, or splint. Nonsurgical treatment is an option, but it will take longer to heal and the risk of repeat rupture is greater. With either type of treatment, you will need a physical therapy program to strengthen your Achilles tendon. It will take 4-6 months to return to your former level of activity. Causes The most common cause of a ruptured Achilles' tendon is when too much stress is placed through the tendon, particularly when pushing off with the foot. This may happen when playing sports such as football, basketball or tennis where the foot is dorsiflexed or pushed into an upward position during a fall. If the Achilles' tendon is weak, it is prone to rupture. Various factors can cause weakness, including corticosteroid medication and injections, certain diseases caused by hormone imbalance and tendonitis. Old age can also increase the risk of Achilles' tendon rupture. Symptoms Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel. An inability to bend your foot downward or "push off" the injured leg when you walk. An inability to stand up on your toes on the injured leg. A popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months. 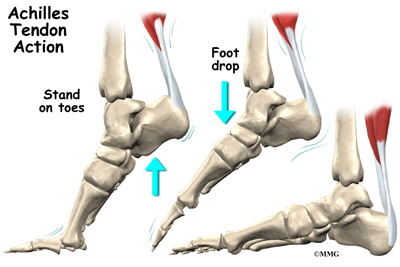 Surgical Treatment Surgery is a common treatment for a complete rupture of the Achilles tendon. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons. Surgical complications can include infection and nerve damage. Infection rates are reduced in surgeries that employ smaller incisions. After treatment, whether surgical or nonsurgical, you'll go through a rehabilitation program involving physical therapy exercises to strengthen your leg muscles and Achilles tendon. Most people return to their former level of activity within four to six months.
Surgical Treatment Surgery is a common treatment for a complete rupture of the Achilles tendon. The procedure generally involves making an incision in the back of your lower leg and stitching the torn tendon together. Depending on the condition of the torn tissue, the repair may be reinforced with other tendons. Surgical complications can include infection and nerve damage. Infection rates are reduced in surgeries that employ smaller incisions. After treatment, whether surgical or nonsurgical, you'll go through a rehabilitation program involving physical therapy exercises to strengthen your leg muscles and Achilles tendon. Most people return to their former level of activity within four to six months.
 A tendon is a band of tissue that connects a muscle to a bone. The Achilles tendon runs down the back of the lower leg and connects the calf muscle to the heel bone. Also called the heel cord, the Achilles tendon facilitates walking by helping to raise the heel off the ground. The Achilles tendon is at the back of the heel. It can be ruptured by sudden force on the foot or ankle. If your Achilles tendon is ruptured you will be unable to stand on tiptoe, and will have a flat-footed walk. It is important to diagnose and treat this injury as soon as possible, to help promote healing. Treatment involves wearing a plaster cast or brace (orthosis) for several weeks, and possibly having an operation.
A tendon is a band of tissue that connects a muscle to a bone. The Achilles tendon runs down the back of the lower leg and connects the calf muscle to the heel bone. Also called the heel cord, the Achilles tendon facilitates walking by helping to raise the heel off the ground. The Achilles tendon is at the back of the heel. It can be ruptured by sudden force on the foot or ankle. If your Achilles tendon is ruptured you will be unable to stand on tiptoe, and will have a flat-footed walk. It is important to diagnose and treat this injury as soon as possible, to help promote healing. Treatment involves wearing a plaster cast or brace (orthosis) for several weeks, and possibly having an operation.
